by Dominic Corva, Social Science Research Director
Today is June 30, 2016, the last day of two eras. It’s the last day of Medical Cannabis as a tolerated parallel cannabis access system in Washington State, and the last day of Phase I of Legal Cannabis in Washington State. Let’s review what’s changing with respect to “Access,” a topic I was asked to address on Sunday, June 26, at the “22 too many” Veterans for Medical Cannabis fundraiser in Olympia.
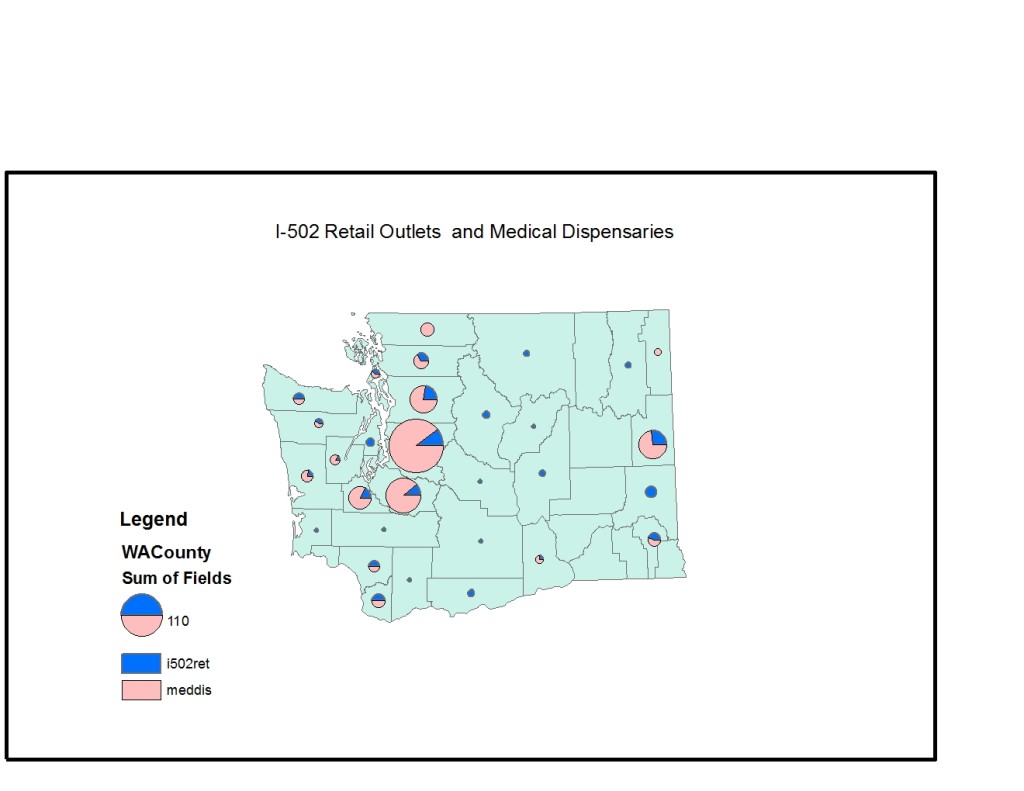
- Storefront access. In the fall of 2015, BOTEC found 404 medical cannabis access points across the state, according to information provided in a public information request. 73 of those were “not verified” although they were listed because their sources, including the City of Seattle, were found to be fairly credible. This number is probably below peak, given that access points began to close starting in July 2015, when SB 5052 went into effect. As of last week’s WSLCB numbers, 179 I 502 retailers accounted for 98% of the previous three month’s statewide revenue. A large percentage of these applied for “medical endorsements,” but let’s just conclude that the state went from 404 access points to less than 179 on the day that the latter was supposed to provide uninterrupted access to the State’s medical patients.
- There is a geographic dimension to this access reduction, which we are working on by mapping those 179 stores relative to those 404 stores. Those maps will be in the forthcoming book, but are not made yet.
- Of those “less than 179” I 502 retail stores that are open and doing substantive business, a very small percentage were actually transitioned from medical cannabis. In Seattle, a recent study found that 3 of the 21 “second wave” retail stores went to existing access points at the locations they used to operate. We found that about 6 more were existing access points that relocated. 9 out of 21 is still an “F” for “Failure to meet the intention of SB 5052 to create a second window for existing medical access points to transition into I 502.” Lawsuits are ongoing. But if the WSLCB Failed in Seattle, where access points had perhaps the most favorable circumstances, we can hypothesize with some confidence that they Failed in the rest of the State. We are adapting the methodology of the CBE report to test that hypothesis, and those results will be published in our forthcoming book.
- If there were at least 400 storefronts a year ago, there are thousands of individual patient grows that are affected. The State may not have liked medical storefronts, but it has never understood the decentralized market that supplied and supplemented it. Home grow access with an affirmative defense has changed dramatically. The upper limit of patient or collective garden home grows was 15 per patient, up 60 plants with 4 or more medical authorizations. Maximum allowable plants (this includes seedlings and clones!) is now 4 or 6 if one registers with the WSLCB. A registered “cooperative garden” can have up to 24 plants, but not only do they have to register they have to master Biotrack, a feat that’s barely been accomplished by I 502 businesses. I have been asking, but to this date I am not aware of a single cooperative garden that has registered with the WSLCB. If you know of one, please let us know.
- Access to authorizations became much more difficult once SB 5052 passed, which intimidated existing doctors who had the expertise and willingness to authorize cannabis for patients. Now, “primary care physicians” have to be involved — and there’s no State requirement that primary care physicians be trained in basic cannabinoid science nor that they be willing to authorize either way. It’s also a class thing: who has primary care physicians in a country when so many have no health care at all, and usually use the health care system only in an emergency?
One could argue that these access concerns are significant only for a small minority of former access point patrons. That’s like arguing that since only a few people have physical disabilities, we don’t need handicap parking or ramps or any of the other ways our infrastructure for the many accommodates the needs of a few. Whether you believe, as our policymakers do, that 90% of medical cannabis patients are “fakers,” or that all cannabis use is medical, the wholesale destruction of access for even that 10% is unconscionable.
It’s unconscionable because it wasn’t necessary, on the one hand, and even if one believes it was necessary, the I 502 system is still too immature and underdeveloped to do it now. The WSLCB proclaims that over 300 retail stores have been approved and we are on our way to 550, but the numbers on the ground say that only 179 retail stores were actually doing business at the beginning of Phase II of Washington State legalization. The State managed to open less than half of its original 335 store allotment over three years, and that includes quite a few “Second wave” retail stores that have been opened in the last 6 months.
Today is a tragedy for common sense and evidence-based policy. You don’t have to like medical cannabis to understand that this is at the very least an extremely premature step, at the very least. SB 5052, the “Patient Protection Act,” has dismantled patient protections without guaranteeing continued patient access, which was just as much a mandate in the law as shutting down storefronts. It’s a bit of a catch-22 for the WSLCB, which was charged with this impossible task (and yes, let’s say the Board and those it answers to supported the general thrust of SB 5052).
What’s going to happen next? A hard legal line has been drawn down the middle of a 20-year social and political phenomenon. In some places, like Seattle, that hard line will be enforced only upon complaint, and it’s likely that civil charges will be preferred to criminal ones. But in many other jurisdictions, those complaints will be aggressive and it will look like prohibition did 20 years ago. It’s also likely, according to former legislator Chris Hurst’s presentation to the Alliance a couple of weeks ago, that complaints will mostly be coming from I 502 retail shops looking to eliminate competition.
There’s no going back, absent some unexpected lawsuit outcomes whose day in court may eventually come. I 502 will grow to maturity over the next few years — I’d say at least 4 before they begin to allocate retail right.
The challenge for those who wield the politics of access is simple. You have to convince the legislature to pass a “home grow” provision, and it doesn’t want to do that for at least 2 years. If patients and patient advocates can unite around this single issue and push the legislature to do something that legislators have clearly stated they don’t want to do, yet, many of the basic issues related to medical cannabis access can be resolved almost entirely. Washington State will eventually have a home grow provision, as all the other legal states do and as California will under AUMA (or legislative action if AUMA doesn’t pass). In the meantime, thousands of previously protected people will in all likelihood live their lives in fear and stress because the law has changed, even if few will get arrested and prosecuted.
It’s that simple. What’s done is done: access for patients has been disrupted against the letter of SB 5052. The politics of access must consolidate around a sane homegrow provision in 2017. There are six months to organize. Go.
Essential reporting thanks Dominic.
Very good article balanced and comprehensive in the face of so many uncertainties created by Washington’s DOH. I personally have a spinal condition and am one of those who can not afford my medical expenses. Growing my own cannabis has been a health godsend and has eliminated opioids from my life. I feel remorse for those who’s potentially fatal health issues that are helped by affordable cannabis, can no longer legally grow their own medicine, in the safety and privacy of their own home.